AI solutions
What we do
Services
Experts in
How we work


Across the healthcare AI assistants we built and launched between 2023 and 2026, development timelines varied significantly. Some assistants reached production 4x to 5x faster than others.
What’s the reason for such a big difference across similar healthtech software development services? Well, there are not one but 3 common reasons — or, it’s better to call them 3 early decisions made on a project: which model the assistant runs on, how the EHR integration is shaped, and whether HIPAA compliance is wired in from the first week or bolted on later.
Speed matters because the value only starts the day it ships. Until then, the team is still doing everything by hand. It handles the patient questions, scheduling, and intake work that doesn't need a clinician, so staff get their hours back. A slow build with compliance bolted on at the end loses that time advantage before the assistant even reaches patients.
So how do you build one that's fast to ship and safe enough for real patient data? That's what we'll cover: where these assistants actually work in healthcare, what results they deliver, and what it takes to put one into a real clinical system, especially once EHR integration, data quality, and regulatory limits come into play. We'll keep it practical, with real decisions we face on our healthtech projects.
An AI-powered virtual assistant in healthcare is software that talks to patients or staff in plain language and acts on what it hears. A patient asks to move an appointment; the assistant checks the schedule, finds a slot, and books it. A nurse asks what a care protocol says about a medication interaction, and the assistant pulls the answer from the clinic's own documentation instead of a generic web result.
The work it takes off a clinician's plate is the repetitive, language-heavy kind: answering the same intake questions, confirming appointments, explaining pre-visit instructions, routing a patient to the right department, logging a symptom report. None of that needs a medical license. All of it eats hours. An AI assistant that handles initial contact and routine follow-ups frees staff to focus on cases that require a person.
What makes it more than a scripted phone tree is NLP, the technology that lets the system read messy human phrasing ("my kid's been running a fever since Tuesday and now there's a rash") and figure out what the person needs. That's the part a rules-based bot can't do.
Knowing where the line sits saves you from building the wrong thing. Here's the honest split on what a medical virtual assistant can and can't do.
What an AI healthcare virtual assistant does well:
Patient engagement. Answering FAQs, sending reminders, explaining instructions, and following up after a visit, in natural language and across channels.
Appointment scheduling and no-show reduction. Booking, rescheduling, and confirming visits, then nudging patients before appointments to reduce the no-show rate.
Symptom intake and routing. Collecting what a patient reports and directing them to the right level of care, which is different from diagnosing them.
Information retrieval. Surfacing the right protocol, policy, or record detail from internal documentation in seconds, not minutes.
Where it's a bad fit:
Diagnosis and treatment decisions. An assistant can run a symptom-checker/triage engine to suggest urgency, but the clinical call remains with a clinician. Crossing that line turns your product into a regulated medical device, which we'll get to.
High-stakes, low-tolerance moments. Anything where a wrong answer causes harm needs a human in the loop.
Cases where the source data is thin or messy. If the clinic's knowledge base is outdated or the records are incomplete, the assistant will be confidently wrong—garbage in, confident garbage out.
The useful way to think about it: the assistant owns the language and the logistics. The clinician owns the judgment.
A production medical virtual assistant is 5 layers stacked together. Each one has a job, and each one hands off to the next:
1. The conversation layer is what the user touches: a chat window in the patient portal, a voice line, or a widget embedded in an existing app. It captures the input and presents the response. Nothing clinical happens here, but it's where the experience is won or lost.
2. The reasoning layer is the brain. This is the LLM plus dialogue management, the part that holds context across a conversation so the assistant remembers what the patient said 3 messages ago and doesn't ask for the same date of birth twice. The LLM interprets intent and decides what to do; dialogue management keeps the session coherent.
3. The knowledge layer is what keeps the assistant honest. Instead of letting the LLM answer from its training data, retrieval-augmented generation (RAG) pulls answers from a controlled source: the clinic's protocols, approved medical documentation, the internal knowledge base. The model reads those documents and answers based on them, which helps prevent it from inventing a dosage or policy that doesn't exist.
Expert take

In medicine, an AI needs to be accurate. The assistants we put into production consistently achieve over 95% accuracy because we focus heavily on the data pipeline that feeds them. We use retrieval-augmented generation to ground the model in real, verified clinical documents. If the knowledge layer is tightly scoped and up to date, doctors trust it. If you skip that step, they’ll abandon the tool the first time it gives them a generic or slightly off answer.
4. The action layer is where the assistant stops talking and starts doing. Booking a visit, updating a record, checking a bill: all of it runs through integration with the EHR/EMR and other systems, using healthcare data standards like FHIR, HL7, or plain REST APIs. Without this layer, you have a chatbot that gives advice but can't touch anything real.
5. The safety layer wraps the whole thing. These are guardrails that block unsafe outputs, content filters, escalation rules that hand a conversation to a human when it gets risky, and audit logging that records who accessed what.
These three terms are used interchangeably in sales decks, which is how you risk overspending when choosing a virtual assistant for healthcare. They're different solutions with different price tags.
An AI chatbot, the simplest tier of chatbot development, reads what the user means, handles questions nobody scripted in advance, and stays coherent when the conversation drifts off-path.
An AI healthcare virtual assistant understands and remembers, runs on an LLM with dialogue management and RAG, and can act within your systems through an EHR integration.
An AI agent goes further, planning and executing a multi-step task on its own.
Here's how they compare on the things that help you make the decision:
| AI chatbot | AI virtual assistant | AI agent | |
| Understands natural language | Yes, basic | Yes, via LLM + NLP | Yes |
| Remembers context | No | Yes, dialogue management | Yes, across multiple steps |
| Pulls from your knowledge base | No | Yes, RAG | Yes |
| Take actions in your systems | Rarely | Yes — connects to EHR systems via FHIR | Yes, multiple actions autonomously |
| Decides its own steps | No | No, one request at a time | Yes, plans and executes |
| Build complexity | Low | Medium to high | High |
| Relative cost | Lowest | Moderate | Highest |
| Good fit for | FAQs, opening hours/business hours, simple routing | Scheduling, intake, patient engagement, record lookups | Prior auth, care coordination, multi-system workflows |
The return shows up in places you can measure. Each one maps to a metric you can track before and after launch:
A front desk spends most of its day on a few repeating tasks: confirming visits, answering "what time is my appointment," rescheduling, and telling patients what to do before a visit. An assistant absorbs that load.
Track 2 numbers. Call deflection rate tells you the share of inquiries resolved without a human. Average handle time tells you how long the calls that still reach staff take. When the assistant clears the routine majority of contacts, both move in your favor.
Every hour not spent on phone triage is an hour back on patients. The mechanism is simple: the assistant takes the language-and-logistics work, and the clinician keeps the judgment work.
This is measurable on internal tools too. An employee-portal assistant we built turns plain-language questions into secure, read-only database queries, answering in seconds what used to take staff hours of manual reporting. In one deployment, that kind of AI process automation saved a team 40+ staff-hours a month, time that went back into work only a person can do.
An assistant answers at 2 a.m. and never puts anyone on hold. For patient engagement, that means reminders that land and follow-ups that happen on time.
The payoff shows up in the no-show rate, since patients get nudged and can rebook in one message. No-shows are lost revenue, so a few points of improvement cover a real slice of the build. Missed appointments cost the U.S. healthcare system an estimated $150 billion a year, and a single no-show costs a physician around $200 in lost income, so even a few points of improvement cover a real slice of the bill.
Over a longer horizon, better post-discharge follow-up can move the 30-day readmission rate. That metric carries real financial weight: the average 30-day readmission costs around $15,200, and readmissions run the U.S. system roughly $52.4 billion a year, which is why it sits at the center of value-based care.
ROI depends on volume. A clinic handling 200 calls a day sees a fast return. A small practice with light volume may not justify the build at all.
It also depends on clean data. An assistant working off an outdated knowledge base creates rework instead of saving it. And slow-moving metrics like readmission rate depend on factors outside the assistant's control, so crediting the full change to one tool overstates the case.
Not every use case fits a half-year timeline. The ones below do, because a virtual health assistant built on well-understood patterns ships faster: language understanding, retrieval from your own documents, and a handful of system integrations.
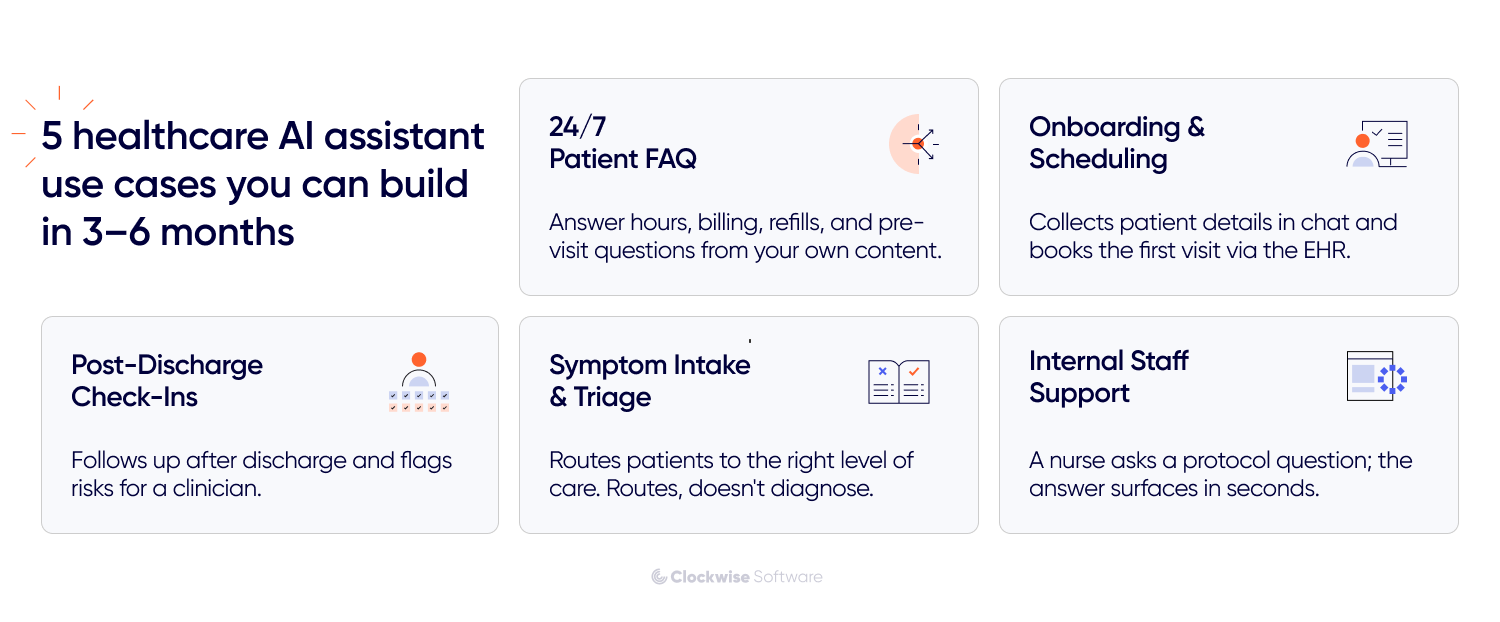
The highest-volume, lowest-risk place to start, and a common entry point for mental health tech platforms too. Patients ask the same questions endlessly: hours, location, what to bring, billing, and how to refill a prescription.
The key is RAG using the clinic's own approved content, so answers come from your policies and documentation rather than the model's training data. Pair it with a knowledge graph if the information has structure worth modeling, like which services map to which departments and providers. This is the use case where the call deflection rate changes the most, because routine questions account for most of the volume.
This is the use case that pays for itself fastest. A new patient messages the assistant, and instead of a form-and-phone-call marathon, the assistant collects their details in conversation, extracts the structured data, and books the first visit.
Here's how it works: NLP reads the patient's free text; named entity recognition extracts the specifics (name, date of birth, insurance ID, reason for visit); and the action layer writes it all into the EHR via FHIR and opens an appointment slot. Scheduling is where the no-show rate gain shows up, since the same assistant handles reminders and one-message rescheduling.
The longest part of this build is the EHR integration and ensuring the extracted data lands in the right fields cleanly. Once that holds, the rest moves quickly.
After discharge, patients forget instructions, skip medications, and miss warning signs. An assistant checks in on a schedule, asks how they're doing in plain language, and uses predictive AI to flag anything that needs a clinician's attention.
This relies on dialogue management to maintain context across days of check-ins, plus RAG for the discharge instructions and care protocols, so the answers match what the patient was told. When a response crosses a risk threshold, the safety layer escalates to a human. The target metric is the 30-day readmission rate, which is why this use case attracts attention from organizations in value-based care.
One honest limit: this assistant supports follow-up; it doesn't replace clinical monitoring. For patients with serious conditions, it's a layer on top of human care, and the escalation rules have to be conservative.
A patient describes what's wrong, and the assistant gathers the details and points them to the right level of care: self-care guidance, a routine appointment, urgent care, or emergency services.
This combines intent recognition to understand the patient's needs, NER to capture symptoms and map them to codes such as SNOMED CT, and a symptom checker/triage engine to suggest urgency. However, it doesn’t diagnose. The moment an assistant outputs a diagnosis or a treatment decision, it can fall under FDA rules for software as a medical device, which is a different regulatory project entirely. Built as a router with conservative escalation, it stays on the safe side of that line.
Pointed at staff instead of patients. A nurse asks what a protocol says about a drug interaction; the assistant pulls the answer from internal documentation in seconds. An administrator asks for a metric, and the assistant retrieves it.
From one of our projects

This pattern actually mirrors an internal tool we built for our own team. We created an assistant that lets users ask plain-language questions, turns those into secure, read-only queries against our internal systems, and delivers answers in seconds that used to require hours of manual lookup. When you bring that exact same approach into a clinical setting, it completely changes how staff surface protocols, policies, and specific record details. It takes a massive administrative burden off the team.
So, you've decided a virtual health assistant makes sense for your case. Now comes the part where most projects either set themselves up to succeed or quietly plant the problems they'll hit 6 months later.
The path below runs from discovery through launch. Each step carries a healthcare-specific catch that a generic chatbot guide skips, and that's where we'll spend the attention. Here's how the build itself goes:
Before anyone writes code, you need a clear answer to one question: Does this use case touch a clinical process? If your assistant only answers billing questions, your risk is low. If it routes patients by symptom or surface care instructions, you're in a different category, and the whole project has to be shaped around that.
This is where discovery earns its keep. At Clockwise Software, we use this phase to map the risk system before committing to a build: what could go wrong, how likely it is, and what each failure would cost a patient or the organization.
For a healthcare AI assistant, that means classifying the use case by clinical impact, identifying where a wrong answer could cause harm, and deciding up front where a human must stay in the loop. Focused discovery saves our clients about $30K, mostly by killing bad assumptions before they become expensive code.
Discovery is how you find out about a compliance gap during the security review, rather than during planning, when fixing it costs 10 times more.
Here's the question that shapes everything downstream: where does your data live, and what kind of data is it?
In healthcare, a large share of information is protected health information, which is subject to strict rules on how it can be stored, processed, and transferred. And it's rarely in one place. It's spread across the EHR, a CRM, a billing system, scheduling tools, RPM solutions, streaming device data, maybe a few spreadsheets nobody admits to. Your AI assistant needs to reach the right data without breaking the rules that govern it.
Compliance is the part you map now. For a US deployment handling PHI, the baseline usually includes:
This step is where we lean on a decade of integration work. Connecting an assistant to live systems without leaking data is the exact problem we've solved across 100+ API integrations, and the patterns carry over: filter sensitive fields before they leave your environment, authenticate every system-to-system call, and log everything.
Which model should you use? It depends on the job, and you're not locked into one. GPT, Claude, Gemini, and healthcare-tuned options like Med-PaLM each have strengths, and the cloud platforms wrap them in compliance-ready services: AWS Bedrock with Comprehend Medical and HealthLake, Azure OpenAI with the Azure Health Bot, or Google Vertex AI with the Healthcare API. Picking the platform often matters more than picking the model, because the platform provides a signable BAA and the security controls already in place.
The architecture pattern that works in healthcare is hybrid. The LLM handles interpretation and conversation, but actions and clinical logic remain under the system's control, not the model's. The assistant can understand that a patient wants to reschedule, but the booking rules, eligibility checks, and escalation thresholds are implemented in deterministic code that you can test and audit. That split keeps behavior predictable, which is the quality that matters most when a patient is on the other end.
Underneath, an event-driven microservices setup lets each component scale and fail independently, and a vector database such as Pinecone, Weaviate, or Milvus powers the RAG retrieval, keeping answers grounded in your documentation. Guardrails wrap the model so it can't produce an unsafe output even if a patient phrases something in a way you didn't anticipate.
Now, how should the assistant actually talk, and when should it stop talking and hand it off?
This is the step teams underestimate. A healthcare conversation isn't a happy path. Patients are stressed, vague, and sometimes describe an emergency in the middle of a routine question. Your flows have to plan for the messy version: what happens when the assistant doesn't understand, when confidence is low, when a patient says something that signals risk.
The rule we design around is conservative escalation. When the assistant isn't sure, or when the conversation crosses a clinical risk line, it routes to a human rather than guessing. You map these decision points explicitly: which intents auto-resolve, which require confirmation, and which trigger an immediate handoff. Getting this logic right is what separates an assistant clinician's trust from one they override and abandon.
Don't build the whole thing first. Build the riskiest slice and prove it works.
A proof of concept lets you test the one thing most likely to sink the project, usually the EHR integration or the accuracy of the assistant on real clinical content, before you've spent the full budget. Our approach to AI development lets us deliver PoCs roughly twice as fast with AI-assisted methods, so you reach a go/no-go decision in weeks instead of months.
For sensitive modules, we build in small, reviewed stages rather than generating everything in one pass, and every piece of code runs through a multi-stage validation filter: automated checks, an independent review in a clean context, manual review by a senior engineer, and functional testing. On a healthcare product, that discipline is what keeps a subtle logic error from reaching a patient. You validate the critical risk here, while it's cheap to fix.
This is usually the longest stretch of the project, so plan for it. Connecting to an EHR such as Epic or Oracle Health (Cerner) via FHIR or HL7 is rarely plug-and-play. Every system has its own quirks, its own version of the standard, and its own approval process, and you only find the real issues when you test against actual data instead of a sandbox.
We never assume an integration will behave the way its documentation claims. We test each connection against real-world conditions, including the edge cases the docs might not have mentioned, because in healthcare, a silent data-mapping error isn't a bug; it's a patient safety issue. Budget more time here than feels necessary. The teams that rush this step are the ones that relaunch.
Launch isn't the finish line; it's the start of the feedback loop. Once the assistant is live, you monitor the metrics that tell you why you built it: call deflection rate, average handle time, no-show rate, and patient satisfaction scores such as CSAT. Audit logging keeps you compliant and provides the conversation data you need to identify where the assistant is weak.
Then you improve. The first version will get some intents wrong, miss some questions, and escalate things it could have handled. That's expected. You feed the gaps back into prompts, retrieval sources, and flows, and the assistant gets sharper over time. A healthcare virtual assistant is a system you maintain, not a feature you ship and forget, and the ones that deliver lasting value are the ones whose owners keep tuning them.
Here's the thing most demos hide. Among current health tech trends, getting a model to hold a smart conversation is nearly solved. The hard part is everything around it: the regulated data, the legacy systems, the clinical stakes, and the people who have to trust it. The complexity of a medical virtual assistant comes from its environment, and that's where projects slow down or stall. Below are the 5 that bite most often, and what to do about each.
This is the constraint that shapes every technical decision you make. The moment your assistant touches PHI, you're operating under HIPAA, and a single careless integration can turn into a reportable breach.
Where it hits the build: compliance limits which models you can use, where data can live, and how it moves. You can't pipe PHI to just any model API. You need a vendor who will sign a BAA, which rules out some options entirely. Data must be encrypted at rest and in transit, and patient identity often must be stripped through de-identification before it reaches an external model.
What to do: treat compliance as a design input from the start. Pick a cloud platform that already offers a BAA and healthcare-grade controls. Filter and de-identify PHI before it leaves your environment. Wire in RBAC and audit logging from the first sprint, so you're never retrofitting access control onto a system that is already shipped. The teams that bolt compliance on at the end are the ones that miss launch dates.
How much should the assistant decide on its own? In most domains, more automation is better. In healthcare, more automation beyond a certain point becomes a patient safety and regulatory problem.
Where it hits the build: if your assistant starts offering anything that looks like diagnostic or treatment advice, it can cross into software-as-a-medical-device territory under FDA rules, which is a long, expensive regulatory path. Push automation too far, and you've accidentally built a regulated medical device. Pull it back too far, and the assistant doesn't save anyone time.
What to do: define the clinical line explicitly during discovery and design conservative escalation around it. The assistant routes, informs, and assists; it doesn’t diagnose or decide. Anything close to clinical judgment is handed off to a human, and the safety layer enforces this automatically. If you do need clinical decision features, scope them as a clinical decision support system with a clinician-in-the-loop, and plan for the regulatory work from the start rather than discovering it later.
Healthcare data is scattered, and the systems holding it weren't built to talk to each other. This is the challenge that eats timelines.
Where it hits the build: your assistant needs data from an EHR like Epic or Oracle Health (Cerner), plus billing, scheduling, and maybe a CRM. Even with standards like FHIR and HL7, every system implements them a little differently, and true interoperability is more aspiration than reality in many organizations. A connection that works in the vendor sandbox often behaves differently against production data.
What to do: budget generously for integration and test early against real data. Never trust that a connection works as its documentation claims, and surface edge cases before launch. Build the integration as the riskiest slice of your PoC, so you know what you're dealing with while it's still cheap to adjust.
An assistant who makes things up is dangerous in any product. In healthcare, a confident wrong answer about a medication or a symptom can cause real harm.
Where it hits the build: a model left to answer from its training data will sometimes invent a dosage, a policy, or a protocol that doesn't exist, and it'll sound authoritative doing it. The risk increases when your source data is messy, outdated, or contradictory, because even a grounded assistant can retrieve the wrong information.
What to do: ground the assistant with RAG over a clean, current, approved knowledge base so it answers from your documents instead of guessing. Add guardrails that block unsafe outputs and a confidence threshold that escalates uncertain answers to a human. And invest in the unglamorous work of cleaning the knowledge base before launch, because a well-built retrieval layer over bad documentation still gives bad answers. Quality in, quality out.
You can ship a technically sound assistant that nobody uses. Adoption is its own challenge, and it's often the one team's plan for the least.
Where it hits the build: clinicians are rightly skeptical of tools that might create extra work or give patients wrong information. If the assistant escalates badly, misreads intent, or feels like a barrier, staff route around it, and patients abandon it. A tool with low trust delivers zero of its projected ROI, no matter how good the engineering is.
What to do: involve the people who'll use it early. A clinical informaticist or a physician reviewer, helping shape the flow of the conversation, catches problems an engineer never would. Be transparent with patients that they're talking to an assistant and make the path to a human obvious and easy. Start with a low-risk use case, prove it works, and expand from there.
So where do you actually begin?
It depends on what you've already got.
A health system planning a virtual health assistant with an in-house engineering team needs something different from a digital health startup tackling wellness app development with an idea and no AI specialists.
If you're not yet sure what to build, what it'll cost, or where the compliance risks sit, this is where to begin. Discovery is the low-risk entry point. We map the use case, classify its clinical impact, surface HIPAA and data constraints early, and build a proof of concept to demonstrate the core idea works — then hand you a realistic plan with timelines and a budget before you commit to full development.
It's also where the money gets saved. For a sensitive healthcare build, that upfront clarity is the difference between a smooth project and a stalled one.
Already have a product team but missing the AI and healthcare-integration expertise? A dedicated team plugs our specialists into your existing setup. You keep ownership and direction; we add the people who've shipped production assistants and handled EHR integrations before.
This fits when you have the roadmap and the in-house knowledge but need to move faster without spending months on hiring.
If you'd rather hand the whole thing to one team and stay focused on your business, we take it end-to-end: discovery, architecture, model selection, integration, compliance, development, launch, and the tuning that comes after. You get a single accountable partner instead of stitching together vendors.
We've delivered 200+ products since 2014 with a 99.89% work acceptance rate, including 10+ healthtech apps running at around 99.99% uptime. That track record is what lets us design an assistant that integrates cleanly with your systems and behaves predictably once real patients are using it.
An AI virtual assistant in healthcare earns its place when it takes routine work off your staff: scheduling, intake, follow-ups, and repeat questions, so clinicians get their time back. The technology is mature. What makes or breaks a healthcare virtual assistant is the environment around the model: the PHI you protect, the EHR systems you connect to, and the trust you earn from the people who use it. Get the early decisions right, and you can ship something real in 3 to 6 months. Start small, ground the assistant in clean data, keep a human in the loop where it counts, and expand from what you can prove works.